
Walsh's Plume Attack Lies About Trans Care: History, Letters, And Informed Consent HRT
Matt Walsh attacked Plume by lying in order to get a letter for gender affirming care. To understand why he did this and why access to care is important, you need to understand the history of care.

Matt Walsh released a hit job on Plume, a gender-affirming care telehealth service, on Wednesday, aiming to halt the service and to initiate investigations into the company. In an effort to achieve this, he enlisted someone to impersonate a transgender adult and lie to healthcare professionals at the organization, with the objective of obtaining a letter for gender-affirming care. Walsh's contention is that transgender healthcare should be less accessible to transgender adults, and his ultimate goal has been the complete eradication of adult transgender healthcare. To fully comprehend his attacks on telehealth, informed consent, and modern adult transgender healthcare, it's crucial to understand the history of this care and the previously common, yet highly detrimental, gatekeeping practices among its providers.
Decades ago, being transgender was treated as a mental health disorder - one in which transgender people were often exposed to brutal treatments when they were not outright arrested and institutionalized. In the United Kingdom in the early 1900s, transgender people were arrested under the Mental Deficiency Act and forced into asylums where they faced electroshock therapy - a practice that continued all the way until the 1960s in both the United States and United Kingdom. None of this worked - these practices resulted in transgender people’s mental health deteriorating and suicidality increasing.
Harry Benjamin Standards Of Care and WPATH
Eventually, the practice of institutionalizing transgender people faded away as therapists determined it was too unethical to attempt to change transgender people’s gender identity. This became replaced with a new form of care: heavily gatekept care run by a select few psychologists around the United States. The new standards of care were developed in 1979. While this was an advancement in that transgender people were no longer forcibly institutionalized, it created its own system of harms for the trans community that it is only recently emerging from.
The new care standards were stringent. Individuals were chosen based on their appearance, with those unable to “pass” as their gender being denied care outright. Moreover, transgender women were required to be exclusively heterosexual, demonstrating attraction solely toward men. Transgender men and nonbinary individuals frequently faced outright rejection. Transgender individuals were compelled to invest thousands in therapy sessions wherein therapists imposed arbitrary personal criteria. For trans women, therapists would ascertain whether they conformed to traditional stereotypes about femininity prior to transitioning and receiving referral letters for their care.
You can see an excerpt about expectations, where trans women who a psychologist judged “could not pass” would not be allowed transition - note that part of “passing” was about fulfilling expectations of women, including mandating that they dated men. See the excerpt:
4.4.4. Principle 12. The best indicator for hormonal and surgical sex-reassignment is how successfully the patient has been in living-out, full-time, vocationally and avocationally, in all social situations, the social role of the genetically other sex and how successful the patient has been in being accepted by others as a member of that genetically other sex

These standards of care would persist until 2011-2013, when several changes to transgender medicine happened at the same time. The World Professional Association of Transgender Health released the Standards Of Care Version 7. No longer did you have to follow rigid guidelines about who you could date, nor did you need to live “as the other sex” for up to two years before getting hormone therapy, a dangerous practice. Likewise, the DSM-V redefined the criteria for gender dysphoria and removed “gender identity disorder” as a mental disorder, stating that the dysphoria itself was the mental diagnosis, and transition is the best form of treatment. However, the most important change from these years was the advent of informed consent gender affirming care.
Informed Consent And Plume
Everything changed in the last 15 years with the introduction of the informed consent model of care. As transgender people gained social acceptance, researchers learned that there were so many more trans people who were closeted than first thought. Due to the increasing demand for gender affirming care, and combined with the fight to end stigmatization of trans identities, doctors started offering care without the need for thousands of dollars worth of therapy sessions and “real life experience” that was completely without evidence.
This turned out to be extremely effective. Informed consent hormone therapy was able to reach patients who previously had been gatekept out of care. No longer did a transgender person have to satisfy a psychiatrist who held to the belief that transgender people must date people “of the opposite gender,” nor did transgender people need to worry about fulfilling gender stereotypes and exaggerating their gender in order to get access to care. Furthermore, a large population of people who did not have the financial resources to obtain care prior were suddenly able to. If you had to move long distances, that care suddenly became accessible regardless of the move. You could also obtain your care privately and present as your gender whenever you were ready to.
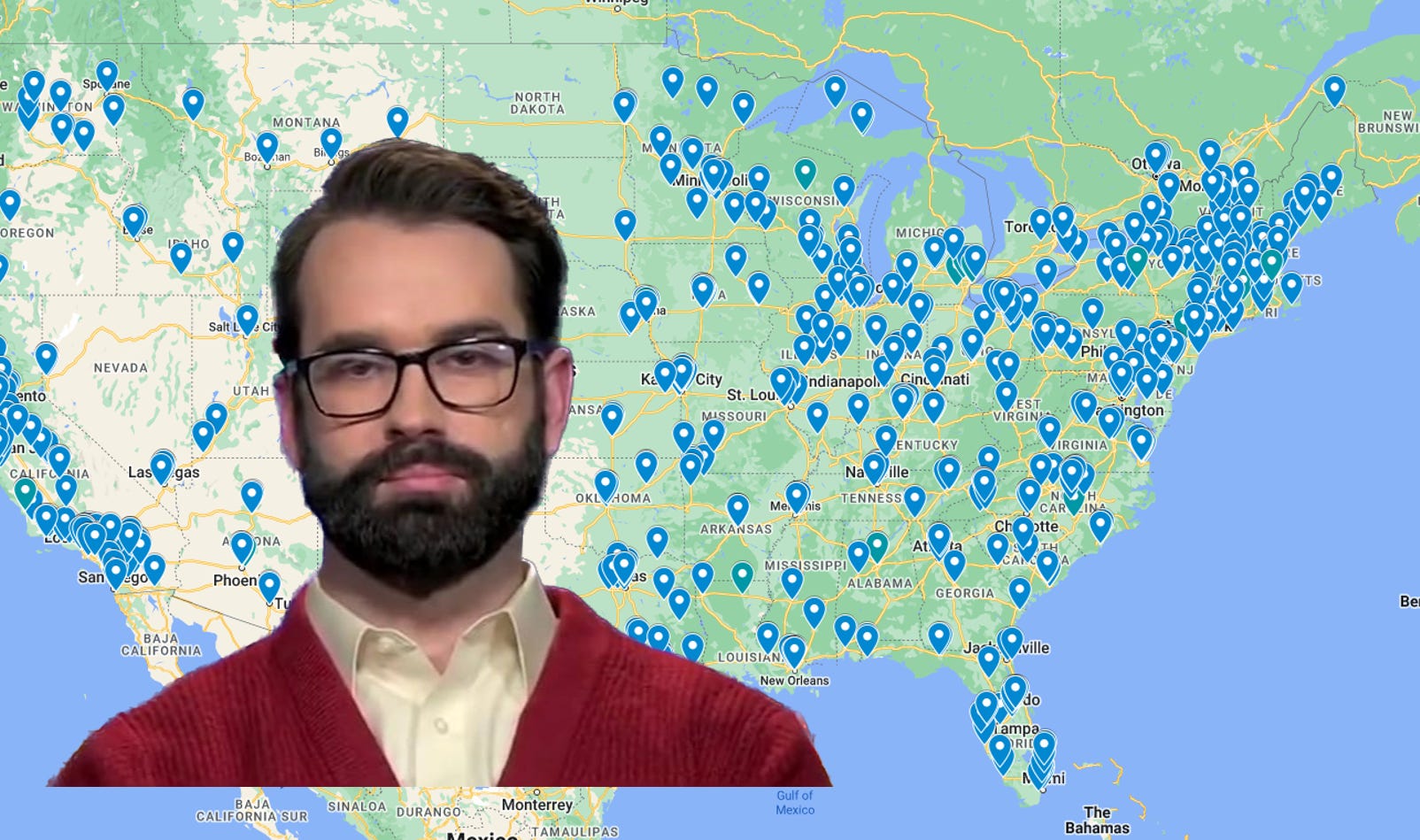
I compiled the informed consent clinics in 2019, which has itself been a resource to the transgender community. My map has been accessed over 5,500,000 times as of the writing of this article, and not a day goes by where I am not thanked by transgender people who used it for their own transition. You can see my map here:

When looking at the map, you can see a couple really important facts about hormone therapy access in 2023. There are several clinics and it is easier to obtain gender affirming care now than it ever has been. Conversely, if one lives in a very rural area, obtaining that care can still be prohibitively difficult. Because many of these clinics require multiple followups, someone living in central Nebraska, for example, may have an extremely difficult time obtaining their care. This is where organizations like Plume and Folx step in.
Companies like Plume and Folx operate via a telehealth on an informed consent basis. They offer virtual appointments with gender affirming care providers so that transgender people can obtain their hormones in places where gender clinics are few and far between. Likewise, they offer letter writing services where transgender people who are seeking further medical transition such as any of the commonly performed transgender surgeries can obtain a letter that meets WPATH Standards of Care, insurance, and surgeon requirements. This is important because gender affirming care can be notoriously hard to get covered, and insurance will reject coverage even for perfectly written letters.
Matt Walsh And The Attack On Plume
Matt Walsh, an anti-trans advocate, tapped his producer to fake being transgender. The producer told the gender affirming care therapist who was writing the letter that he had been on hormones for more than two years and lived as a woman for six. The producer was requesting a letter for an orchiectomy - a commonly performed surgery for transgender people. In order to be approved for the surgery, the letter needs to very closely match the WPATH guidelines, insurance guidelines, and guidelines that will be accepted by doctors. These letters are hard to write and only people who have studied the specific things that need to be in them can write them effectively.
Walsh’s fake patient reported living as a woman for six years and taking hormones for two. These presenting facts fall well within the guidelines for surgery. We would expect all trans women who seek care with those facts to be approved for such a procedure.
Matt Walsh presents what he claims is a damning piece of evidence that these letters are written fraudulently: in an intake form, the producer says they have never had dysphoria lasting for more than six months. See the intake form answer from Matt Walsh here:

Walsh is correct that the standards of care require that dysphoria lasts six months or more. However, Walsh gets one thing absolutely and fundamentally wrong: many patients do not understand what counts or qualifies as “gender dysphoria.” The therapist’s job in letter writing and evaluating is not to automatically just regurgitate what the patient says - rather, the therapists job is to contextualize the patient’s experiences with the diagnostic criteria and medical requirements to obtain care. In the case of Walsh’s fake patient, the patient absolutely meets the guidelines for gender dysphoria.
In the letter that was written, we learn that Walsh’s producer stated that they have lived as a woman for six years and have been on hormones for two. We also learn that they are attempting to obtain an orchiectomy, which means they are experiencing an incongruence between their primary and secondary sex characteristics and their gender identity. See the letter:

The reality of the situation is that regardless of the patient answer in the box on “has this dysphoria ever lasted more than 6 months,” the patient actually fulfills several of the diagnostic criteria for gender dysphoria - only two of the criteria need to be fulfilled, and they fulfill four. See the diagnostic criteria:

An individual who has been living as another gender for six years absolutely fulfills criteria D and E. An individual taking hormones for two years absolutely fulfills criteria B and C. They fulfill all of the diagnostic and insurance requirements with room to spare. However, Walsh believes that the patient’s self reported answer on dysphoria should override that. We know, though, that the patient is seeking gender affirming care while already presenting four criteria met - to deny that care would go against medical guidelines. The “slam dunk” that Walsh believes he has produced is only because he is relying on his audience’s ignorance of what gender dysphoria actually is in a clinical setting.
Walsh likely knows this though. He has repeatedly advocated for an end to all gender affirming care. After some success at banning care for transgender youth in multiple states, it is clear that he is looking at transgender adults as a new target. He likely knows that it will be very hard to justify banning all adult care, so instead, he has had his eyes set on one of the biggest adult care providers. By drumming up false controversies, similar to tactics used against Planned Parenthood abortion clinics, he can spawn investigations and new legislation to restrict adult care.
We are seeing the very beginnings of this in Florida, where 80% of all transgender care was criminalized through a ban on nurse practitioners practicing that care. The remaining 20% of those obtaining care in Florida are similarly seeing bans, as a mandatory medical disinformation form that has yet to be published is creating a delay for transgender adults. Walsh unsurprisingly supports Florida’s decision to ban most adult care in his tweets.
Nonetheless, his fake “expose” of Plume led to an extreme reaction among the right wing, anti-trans twitter space as well as anti-trans public officials and presidential candidates. Elon Musk replied that it is “incredibly disturbing.” Utah and Tennessee’s attorneys general hinted at investigations. Both Donald Trump and Ron DeSantis’ presidential campaigns responded with statements against gender affirming care.
If Walsh successfully dismantles care provided by organizations like Plume and Folx, large areas of the country will once again face a situation where transgender individuals living far from major cities cannot access their care, leading to medical detransition. Furthermore, Walsh is undeniably attacking the entirety of informed consent adult care in his remarks, plainly opposing the concept that adult transgender patients can direct their own care under medical oversight. The elimination of this resource could reintroduce extreme gatekeeping for transgender adults. Those lacking resources could find themselves completely shut out from care once again. The aim, as others in his organization have voiced, is the elimination of transgender individuals and a regression to a time when medical care was not universally available to all transgender individuals.
He is a self serving uneducated scumbag who will say anything to promote himself! He lies constantly, but he has an equally uneducated audience. We need a spokesperson! Let me be it. How do I get there?
Researching this tonight rather than getting sleep like a sensible person I find that Matt may have admitted to a crime https://www.fbi.gov/investigate/white-collar-crime/health-care-fraud