
New NHS England Review Excluded 97% Of All Trans Studies To Say Care Doesn't Work
The new review has led to a ban for HRT through the NHS England system under the age of 18.


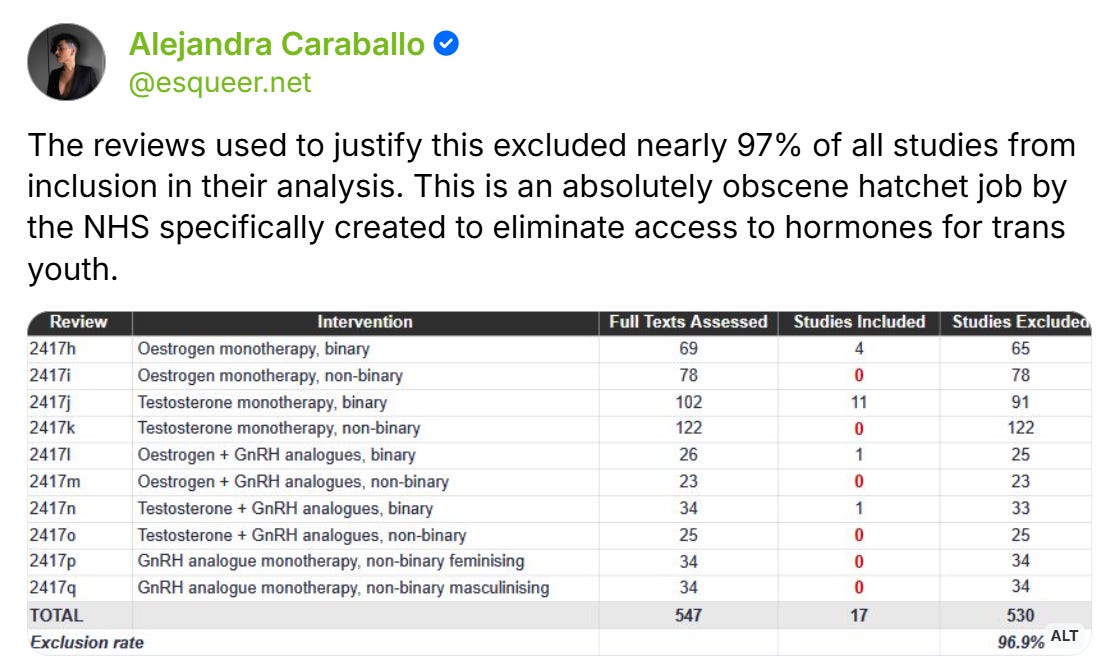
On Monday, NHS England published 10 evidence reviews purporting to show that the quality of evidence for hormone therapy for transgender youth is low. The reviews were released alongside an announcement that the healthcare system would be banning new hormone prescriptions for transgender youth under the age of 18. But upon closer examination, the evidence reviews appear to be an extreme example of politically-manufactured science—similar to other reviews that have come out of the UK in recent months to provide political justification for banning gender-affirming care. Across the 10 reviews, 547 full-text screenings resulted in just 17 studies included—a staggering 97% exclusion rate. The reviews used exclusion criteria designed to guarantee that result, discarded some of the most significant transgender care studies published in the last decade for nonsensical reasons, and then reached what appears to be a predetermined conclusion: that there is insufficient evidence that hormone therapy for trans youth works.
In the last decade, there have been dozens of studies showing the positive impact of gender-affirming care for transgender youth—in particular, hormone therapy’s effects on reducing depression, anxiety, and suicidal ideation. On the flip side, there has been a strong push to ban gender-affirming care for trans youth and even adults among anti-trans activists in the United Kingdom. So researchers at NHS England apparently found a way to get around the evidence rather than contend with it. Instead of conducting one or two comprehensive reviews of the evidence for hormone therapy in trans adolescents, they split the question into 10 separate reviews—fragmenting by exact pharmacological combination (estrogen alone, testosterone alone, estrogen with GnRH analogues, testosterone with GnRH analogues, GnRH analogues alone) and then splitting each of those again by whether the patient identified as binary or non-binary. The result was 10 artificially narrow reviews, each searching for a hyper-specific patient population that most published research was never designed to capture. Studies that didn’t perfectly match a given review’s narrow criteria were excluded—even if they contained data directly relevant to the question of whether hormones help trans youth. As a result, 97% of full-text screenings were excluded from the results.
The Cochrane Handbook, widely considered the gold standard for systematic review methodology, explicitly warns against this approach: “Splitting comparisons carries its own risk of there being too few studies to yield a useful synthesis.” The Handbook advises review authors to use “broader questions” that “may be useful for identifying important leads” in cases where splitting comparisons yield too few useful studies. NHS England did the opposite. In research methodology, this kind of unjustified fragmentation is known as “salami slicing”—a practice that, according to a 2017 analysis in Developmental Medicine & Child Neurology, “encourages other forms of malpractice” and results in “scientific progress stalled and the literature polluted.” By splitting the evidence into 10 pieces, NHS England guaranteed that each piece would be too small to support a conclusion—and then cited the smallness as the reason to ban care.
In doing so, the researchers excluded some of the most impactful studies on transgender youth care published in the last decade. The largest NIH-funded prospective study of trans youth ever conducted—Chen et al 2023, published in the New England Journal of Medicine with 315 participants—was excluded from all ten reviews because it studied trans youth as a cohort rather than separating them by exact hormone regimen. Tordoff et al 2022, published in JAMA Network Open, which found 60% lower odds of depression and 73% lower odds of suicidality among trans youth receiving hormone therapy, was likewise excluded. Perhaps most damningly, the reviews systematically excluded the Dutch Protocol studies—the research that forms the foundation of the modern standard of care for transgender adolescents worldwide.
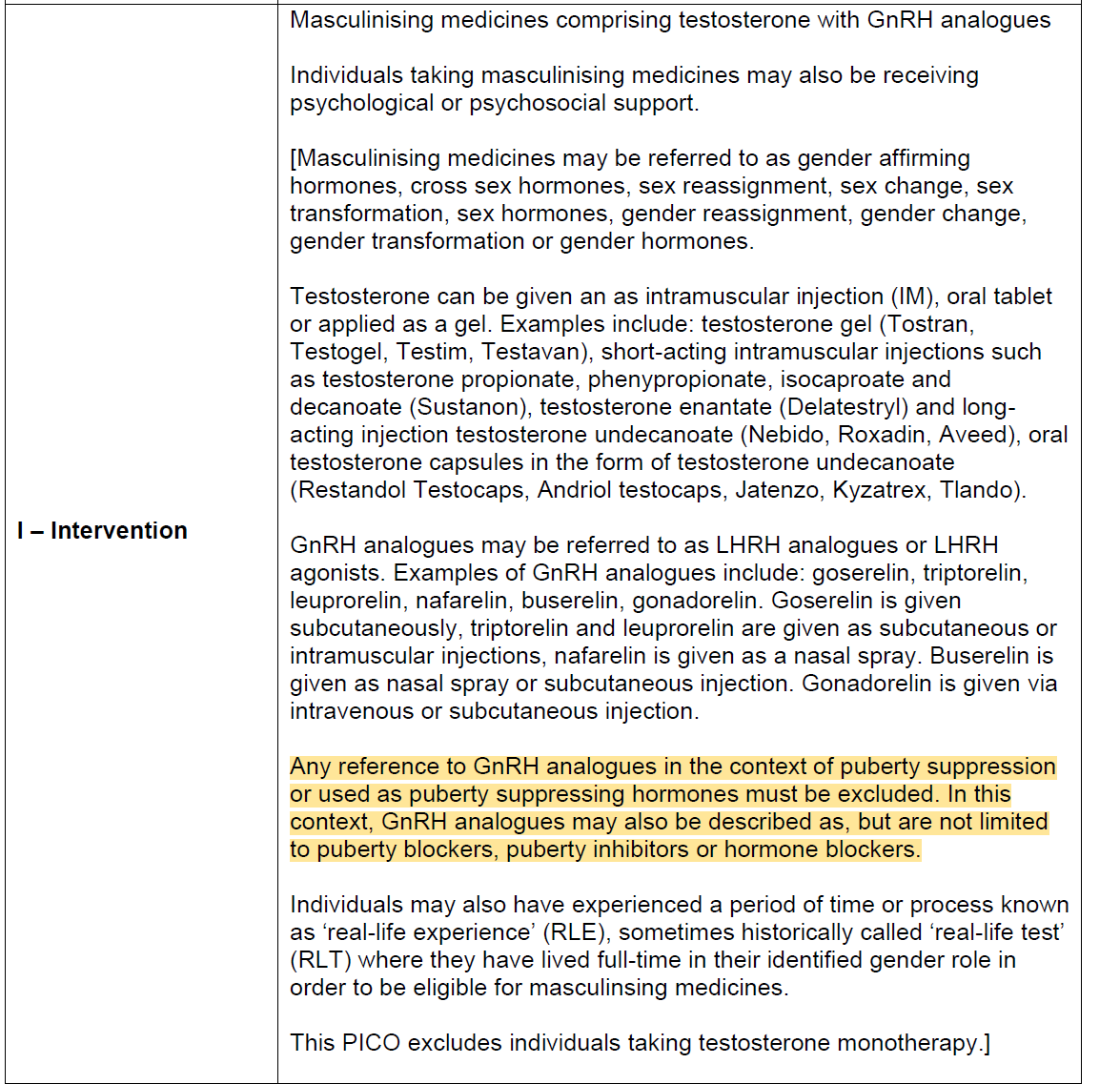
The Dutch Protocol involves prescribing GnRH analogues (puberty blockers) first to suppress puberty, then adding hormones later. When hormones are introduced, the GnRH analogues are sometimes continued alongside them—the blocker keeps suppressing the body’s natural hormones while the prescribed estrogen or testosterone does its work. This overlap period means patients are on both GnRH analogues and hormones at the same time. That is the “combination therapy” the reviews claim to examine. But the reviews inexplicably excluded every study where GnRH analogues were initiated for puberty suppression—even if the patient later ended up on exactly the combination of drugs the review was searching for. The monotherapy reviews excluded these studies because patients had received puberty blockers. The combination therapy reviews also excluded them, because the GnRH analogues were originally started for puberty suppression rather than started at the same time as hormones. NHS England’s own data, cited in the reviews themselves, confirms that 98% of its patients followed the very pathway every review was designed to exclude.
See the exclusion criteria for “Masculinizing medicines comprising testosterone with GNRH analogues”, which explicitly excludes any studies that reference GnRH analogues in the context of puberty suppression or used as puberty blockers:
The reviews then use their manufactured scarcity to make sweeping claims about the "low quality" of evidence for hormone therapy. Even after excluding 97% of all screened studies, several of the surviving studies still showed statistically significant benefits—including reductions in anxiety and depression. To discount those findings, the reviewers turned to the GRADE system, a framework that rates the certainty of evidence on a scale from high to very low. Under GRADE, observational studies—which make up the vast majority of all pediatric research—automatically start at "low" and are routinely downgraded further. Every surviving study was rated "very low certainty."
But Gordon Guyatt, the McMaster University researcher who literally coined the term "evidence-based medicine" and helped develop the GRADE framework itself, has forcefully rejected this use of his work. In a 2025 interview with STAT News, Guyatt called using systematic reviews to justify banning gender-affirming care "egregious and unconscionable." As Guyatt has explained, a low GRADE rating is not a finding that a treatment doesn't work—it is a technical classification reflecting the type of study available, not the direction or strength of the results. Observational studies, which form the backbone of nearly all pediatric medicine, automatically receive low GRADE scores regardless of their findings. Importantly, over 90% of medicine lacks “high-quality evidence” as classified by the GRADE system, which explicitly does not bar medical care that relies heavily on individualized approaches. This is especially true among pediatric populations, where most evidence is “low quality” due to safeguards around experimentation on youth.
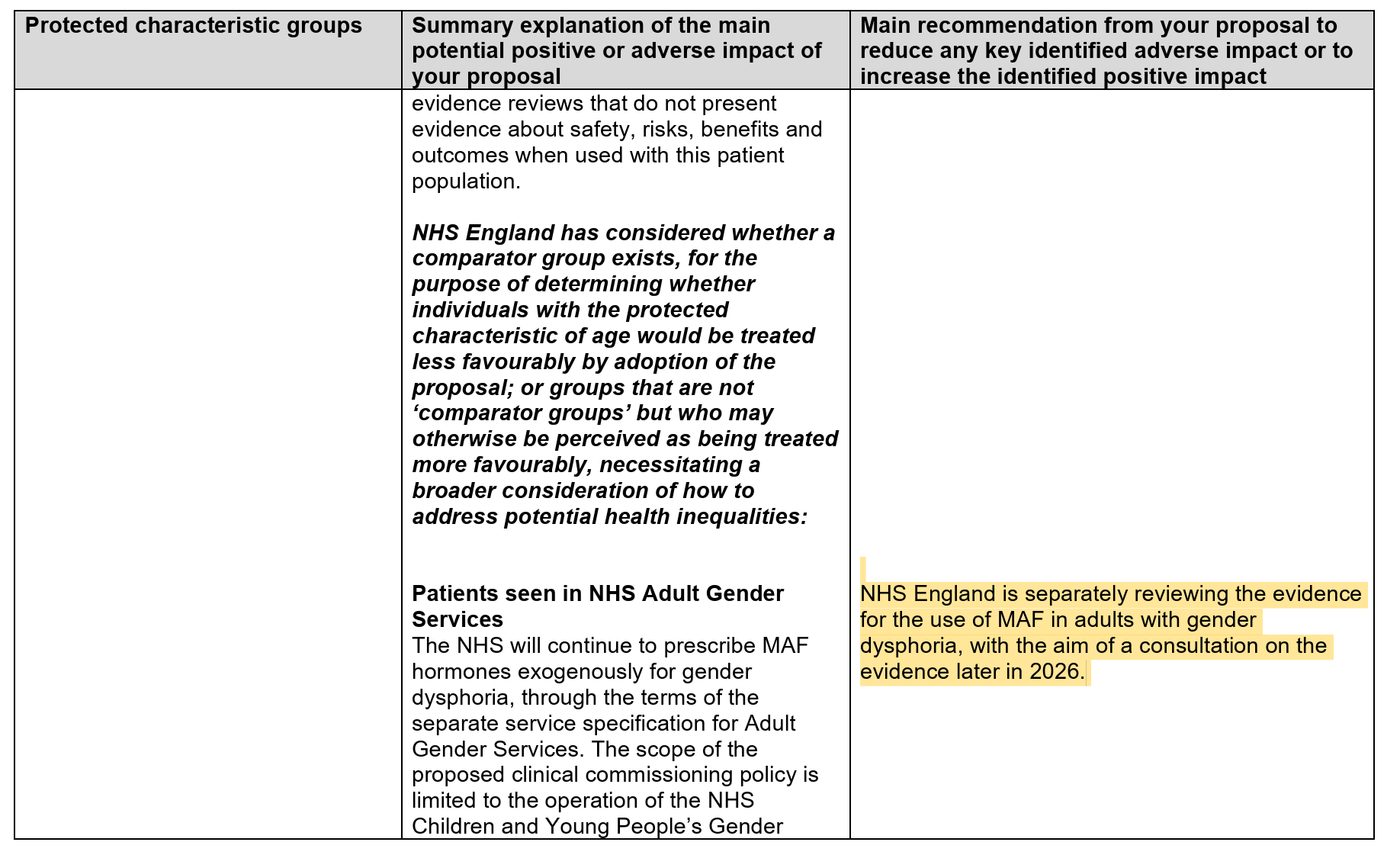
The studies were released alongside an announcement that NHS England would be pausing all new prescriptions for gender-affirming hormone therapy for people under the age of 18. This is a significant escalation in the United Kingdom, which had until now still allowed hormone therapy for 16- and 17-year-olds but had already instituted a ban on puberty-blocking medications in December 2024. Worse, buried in the equalities impact assessment accompanying the reviews, NHS England reveals that a similar process is already underway for adult care. The document states that NHS England is "separately reviewing the evidence for the use of MAF in adults with gender dysphoria, with the aim of a consultation on the evidence later in 2026." If that review follows the same methodology, it could be used to restrict or eliminate gender-affirming hormone therapy for trans adults in the UK as well.
It seems likely that these reviews will be cited in other countries around the world to justify their own regressive policies—just as the Cass Review was before them. The Cass Review, which used similarly flawed methodology to justify banning puberty blockers in the United Kingdom, has since been cited by Republican lawmakers in the United States, referenced in briefs before the Supreme Court in United States v. Skrmetti, and used to greenlight state-level bans on gender-affirming care across the country—despite being criticized by the Yale Integrity Project and major global medical organizations that have examined it. These 10 reviews are not science. They are the machinery of a government that has decided to eliminate transgender healthcare and is working backward from that conclusion. The United Kingdom continues to serve as the launchpad for anti-trans pseudoscience worldwide.
They had to look long and hard to find the studies to support the results they wanted and to support their confirmation bias.
Backed and paid for, I suspect, by a billionaire TERF and transphobic children's book writer, too!
The whole of the gender critical edifice, is fraud from beginning to end. Whether in the UK or US or anywhere, it is all only fraud.
Cass if I recall lied about collaborating with transphobes in Florida in her crafting her fraudulent "Review". The Hague is for her.
What we must bring to bear here in the US are federal anti-discrimination, right protections laws such as 42 U.S.C. § 1983, 18 U.S.C. § 241, & 18 U.S.C. § 242. It must become a part of the Dem Party Platform.