
Fact Check: Trump's HHS Review On Trans Care Filled With Pseudoscience, Pushes Conversion Therapy
The review, which was made possible by an executive order calling transgender healthcare "mutilation," reached its predetermined conclusion on its May 1st publication date.

On Thursday, May 1, the Trump administration’s Department of Health and Human Services, now helmed by Robert F. Kennedy Jr., released a report masquerading as science but serving as a blunt instrument of ideological warfare against transgender youth. Commissioned under Trump’s Jan. 28 executive order, the report’s conclusions were preordained, its framing designed to validate a political agenda rather than present credible research. It names no authors, has no peer-reviewed process, and bears no hallmarks of legitimate scientific inquiry—just a faceless document no one was willing to claim. Among its recommendations: conversion therapy for trans youth, the reclassification of social transition as medical treatment, and an absurd assertion that transgender care should be judged not by patient well-being or satisfaction but by “employability” and the presence of “romantic partners.”
At more than 400 pages, the document is poised to draw a wave of fact-checks and scientific rebuttals. The American Academy of Pediatrics has already issued a sharp condemnation, calling it “inaccurate,” “misleading,” and a distortion of “the current medical consensus.” This fact check won’t capture every falsehood in the report—there are hundreds—but it will examine some of its most egregious and harmful pseudoscientific claims.
Before delving into the document’s most egregious factual distortions, it’s worth emphasizing that it has no listed author and bears none of the hallmarks of scientific rigor. There is no evidence of peer review. Instead, the report reads less like a medical analysis and more like an anti-trans screed—politicized, inflammatory, and devoid of scholarly grounding. Tellingly, transgender researchers have already unearthed EXIF data embedded in the file, revealing that the document’s compilers include Alex Byrne, an anti-transgender philosophy major, and two political consultants—not scientists, and certainly not experts in gender-affirming care.
That said, regardless of their backgrounds, their assertions can and should be challenged. This fact check will endeavor to do just that.
Claim: Transgender healthcare should be judged based on how “unemployed” a person is or how many “romantic partners” they have.
Fact: Transgender healthcare, like all medical care, is judged according to the impact it has on patient health as well as patient satisfaction with the care received.
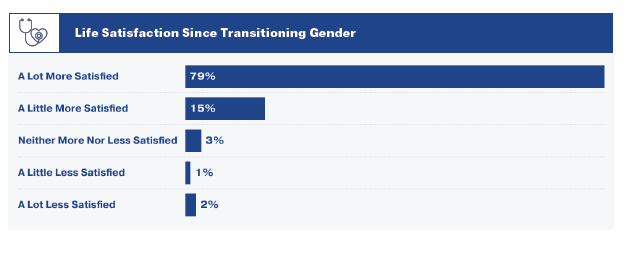
Very early in the review, the unnamed reviewer must contend with the fact that gender affirming care has high satisfaction rates. In recent years, many reports have emerged showing high levels of satisfaction and low levels of detransition for transgender people. A recent report in the 2022 US transgender survey shows that out of 90,000 transgender people, less than 1% report feeling less satisfied after beginning gender affirming hormone therapy, with the vast majority feeling “a lot more satisfied.”
Detransition appears to be similarly rare. One recent study out of Australia found complete data on 548 of 552 transgender patients and discovered only 1% of transgender youth detransitioned over several years before being transferred to adult services. Another study showed that transgender youth are stable in their gender identity 5 years after transitioning, with only 2.5% reidentifying as their assigned sex at birth. Even the Cass Review found less than 10 detransitioners out of the 3,000 trans youth active patients or waiting list patients in England.
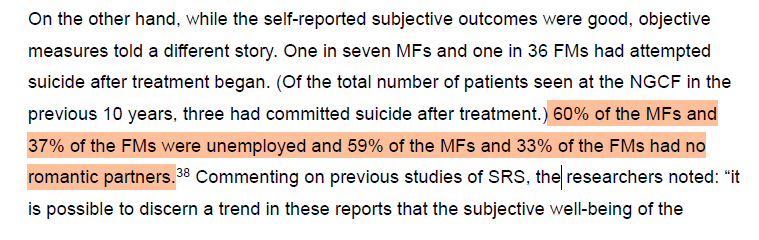
Anti-transgender activists have long struggled to rebut the high satisfaction rates reported by those who receive gender-affirming care, and the authors of this report are no exception. Unable to discredit those numbers directly, the reviewer pivots instead—arguing that satisfaction is irrelevant because, “objectively,” transgender people are doing “poorly.” The evidence? A single 1988 study—nearly 40 years old—claiming that 60% of male-to-female and 37% of female-to-male transitioners were unemployed, and many lacked romantic partners. These are held up as “objective measures.”
It is important to note that all of these potential outcome measurements may be heavily influenced by transphobic sentiments in society, especially in 1988. Should transgender people be judged on their ability to be "employed" or their romantic partners, their own discrimination may then be used against their ability to access medication. According to the Advocates 4 Transgender Equality, more than one in four transgender people have lost a job due to bias, and three-quarters report experiencing workplace discrimination. Therefore, it is inaccurate to blame transgender people and their medication for what appears to be an issue with societal discrimination.
The idea that transgender people are “unreasonably” or “suspiciously” happy in the face of poor “actual life circumstances” has a long history in the mistreatment of transgender people. In 1979, Conservative Activist doctor Paul McHugh abruptly ended gender affirming surgeries at Johns Hopkins. He based the decision on a study that judged the effectiveness of transition with employment status, legal difficulties, and entering into relationships (notably, points were deducted for transgender people entering into gay relationships). Surgeries have since restarted, with Hugh’s history being described as “a long shadow” cast on Johns Hopkins Hospital.
Claim: European countries are pulling back on transgender healthcare.
Fact: The talking point that Europe is “pulling back” on transgender care is now thoroughly outdated. In fact, several European nations have moved in the opposite direction. France, Germany, Austria, and Switzerland have all released recent reports that directly contradict the rationale behind documents like the Cass Review—and this freshly released Trump administration review.
In recent years, U.S. politicians have selectively framed European healthcare policies to justify restrictions on transgender care, seizing on a handful of conservative policies to claim that “Europe is pulling back.” The most extreme example, the United Kingdom’s Cass Review, has been wielded to justify a near-total ban on puberty blockers and even cited in U.S. Supreme Court arguments. This document makes a similar argument, claiming that European countries, starting in 2020, began reversing course on gender affirming healthcare, with the culmination of such reversals being the Cass Review.
This claim is no longer true. Since the Cass Review’s release, numerous European countries and medical associations have actually changed course. In December 2024, the French Society of Pediatric Endocrinology and Diabetology released a groundbreaking national medical consensus on transgender youth care. Importantly, the French guidelines now recommend in favor transgender youth care, denounce a “wait-and-see” approach for transgender adolescents, and promote individualized care for every transgender patient - a stark contrast with the Trump HHS Review. Similarly, new medical guidelines from Germany, Austria, and Switzerland reaffirmed the importance of gender-affirming care for transgender youth and issued sharp critiques of the Cass Review, calling out its severe methodological flaws and misrepresentations - misrepresentations the Trump HHS review shares.
The Trump HHS review acknowledges these updated European guidelines but dismisses them as merely “sparking considerable debate.” It makes no effort to engage with their findings point by point. Instead, it glosses over their conclusions, deriding them as products of WPATH—the World Professional Association for Transgender Health—and falsely claiming they are not evidence-based. In reality, these guidelines are backed by extensive, unbiased citations, the endorsement of major medical organizations, and transparent authorship—none of which can be said of the Trump HHS review.
Claim: Transgender people may actually just be gay, and transitioning is a form of “conversion therapy.”
Fact: Gender and sexuality are different, many transgender people identify as gay or bisexual after transition, and gay acceptance is higher than trans acceptance.
The claim that transgender people are “actually just gay” is one that has been made repeatedly by those opposed to gender affirming care, and one that has been repeatedly debunked. The claim is that people transition for “social acceptance,” a claim that stretches credulity given differential acceptance of gay and transgender people.
This is not born out by factual research and common sense on LGBTQ+ prevalence among transgender people. Attitudes towards transgender people tend to be “significantly more negative” according to an article in the International Journal of Environmental Research and Public Health. This contributes to a much higher rate of violence and discrimination. Many transgender people, such as celebrity Laverne Cox, report that the most common response to coming out is, “couldn’t you have just been gay?”
According to the 2012 National Transgender Discrimination Survey, most transgender people identify as lesbian, gay, bisexual, or queer after transition. If transition was being used to “cure” being gay, it is a startlingly ineffective cure.

Claim: Transgender youth are more common today because of a mass “social contagion,” and transgender people are experiencing rapid-onset gender dysphoria.
Fact: Transgender people often know about their gender identity for years before coming out, which can appear “rapid.” The increase in recent years is not due to “contagion,” a discredited theory, but rather, increased social acceptance of transgender people.
In several instances, the report pushes "Rapid Onset Gender Dysphoria" and "social contagion" as potential reasons for the apparent increase in transgender individuals in recent years, raising concerns that these individuals will detransition. A letter from over 60 psychological organizations, the coalition for the Advancement & Application of Psychological Science calls for the elimination of the term, stating, “There are no sound empirical studies of ROGD” and “there is no evidence that ROGD aligns with the lived experiences of transgender children and adolescents.”
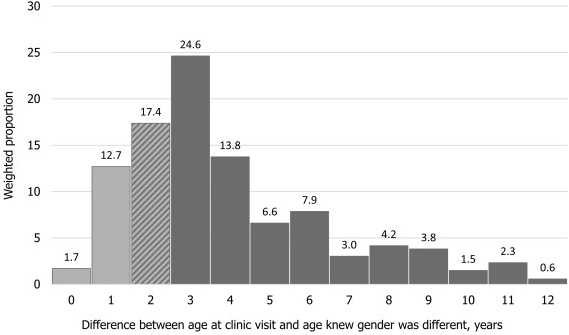
A study in the prestigious journal Pediatrics entirely debunked the concept of ROGD, determining that most transgender people know their gender identity for years before they come out and seek treatment for gender dysphoria. When transgender people finally do come out, many are overjoyed to finally reveal their true self to the world around them - to others, however, the process may seem “rapid.” To ascertain whether transgender identification occurs "rapidly," researchers directly asked transgender teenagers: "How long have you known you were transgender?" They discovered that on average, transgender people know their gender identity for four years before first coming out and presenting for treatment.
In the early 1900s, the rates of left-handedness hovered between 3-4%. Left-handedness rates then “skyrocketed” to 12% where it has leveled off ever since. This was, of course, not caused by a “massive social contagion” of left-handedness. Rather, increases in acceptance led to people feeling comfortable using their left hand. In the 1940s, anti-left-handedness researcher Abram Blau decried the “cultural influences” of left-handedness and the “progressive campaigns” of allowing the child “to be free to choose the side for himself.”
In an article released in 1979, Dr. Bernard McKenna said of the growth of left-handedness, "We used to call everybody a deviant who didn't conform. We just eventually learned better. There was recognition by medical authorities that left-handedness was normal and that tying the hand up in a child often caused stuttering."
Sound familiar?
You can see the growth in left-handedness here:

Claim: Psychiatric care for transgender youth is not conversion therapy. Conversely, conversion therapy to treat gender dysphoria can work.
Fact: Conversion therapy is enormously harmful for transgender youth, and psychotherapy alone has never been shown as effective in “curing” gender dysphoria.
The review flounders when attempting to present viable alternatives to gender-affirming care—chief among them, psychotherapy. There is no comprehensive evidence that talk therapy alone can treat gender dysphoria. On the contrary, the documented harms of conversion therapy are extensive: LGBTQ+ youth subjected to it are more than 2.5 times as likely to report multiple suicide attempts in the past year. The report attempts to have it both ways—insisting that psychotherapy for gender dysphoria isn’t conversion therapy, while also suggesting, in the same breath, that conversion therapy (“psychotherapy” or “psychiatric care” in the report) might actually be effective in curing gender dysphoria.
The report leans heavily on the favored approach for anti-transgender activists called “gender exploratory therapy,” a new type of conversion therapy with a misleading name which seeks to persuade transgender individuals that their gender identity stems from anything but authentic transness. While this form of therapy purports to “help transgender youth explore their gender identity,” the actual intent is far more sinister. In these sessions, therapists repeatedly "explore" a seemingly endless list of possible "reasons" for being transgender, despite lacking evidence that any specific factor "causes" someone to be trans. Crucially, there's no scenario where being transgender is acknowledged or accepted. Letters endorsing hormone therapy for trans youth are never issued, and often their social transition is not allowed. Instead, the therapy aims to psychologically manipulate teenagers, sometimes for years, until they abandon their pursuit of transitioning. This stance is further highlighted by several practitioners who assert that transgender individuals shouldn’t be allowed to transition until the age of 25.
The Gender Exploratory Therapy Association frequently denies that it engages in conversion therapy. They assert that their therapeutic approach is “neutral in nature” and “does not prejudge outcomes.” Yet, this association opposes bans on conversion therapy, submits public comments in favor of blocking Title IX protections against gender discrimination for trans students, and its official account has been observed endorsing tweets like “trans healthcare is the latest in a long line of medical fads.” Such actions hardly mirror the claims of a “neutral, non-prejudiced” entity or neutral approach.
The Trump HHS report will undoubtedly face withering scrutiny in the weeks and months ahead. Similar documents have already been dismantled by leading medical institutions, including the Yale Integrity Project, for their distortions and bad-faith science. While this fact check is not exhaustive, it exposes several of the report’s most dangerous falsehoods and pseudoscientific claims. For those continuing to track its fallout, I’ll be cataloging additional errors and misrepresentations in an ongoing thread on Bluesky.
This just in, depressed people are more likely to be single and unemployed. Surely it will be solved if we take away their meds and let them get more depressed.
Thank you for taking the time to write all this out so clearly. I am sharing with my colleagues who are mentors for the WPATH Global Education Initiative (i.e., we train therapists and medical providers).